Clinical details:
30 years old male patient came with c/o watery discharge from left nasal cavity - 3 years duration
H/O Road traffic accident 3 years back following which watery discharge started.
H/O meningitis 2 years back for which he was treated.
H/O Head ache on and off ++.
H/O Road traffic accident 3 years back following which watery discharge started.
H/O meningitis 2 years back for which he was treated.
H/O Head ache on and off ++.
On examination:
Watery discharge was seen flowing out of left nasal cavity. It was more pronounced when the patient bent down.
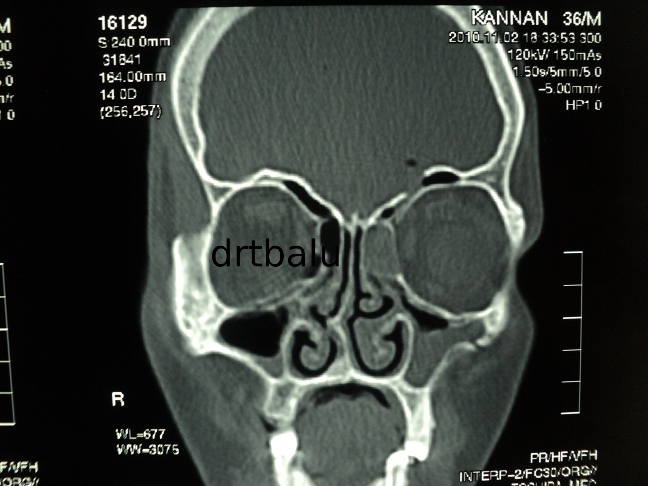
Imaging:
CT paranasal sinus showed fracture involving the posterior table of frontal sinus with evidence of pneumatocele in the left
frontal lobe.
frontal lobe.
Management:
Since the fracture was present laterally in the posterior table of frontal sinus external approach was preferred.
Bicoronal approach was used to expose the anterior table of frontal sinus.
The incision begins in the preauricular crease at the level of tragus and traverses the scalp 3-4 cms behind the hair line.
The incision is carried down through the galea to the loose alveolar plane above the calvarial periosteum and the deep temporal
fascia and the flap is elevated anteriorly until approximately 2cms above the supra orbital rims. At this point the periosteum is
incised and the dissection is continued in the subperiosteal plane. The supraorbital neurovascular bundles are protected.
Laterally the dissection continues in the subgaleal plane up to 1-2 cms above the zygomatic arch. The deep temporal fascia
is incised at this point and the dissection continues deep to the temporal pad of fat over the temporalis muscle and the investing
fascia. The deep temporal artery perforators should be protected if not this could lead to a hallowing in the temoporal area due
to wasting of temporalis muscle.
The incision is carried down through the galea to the loose alveolar plane above the calvarial periosteum and the deep temporal
fascia and the flap is elevated anteriorly until approximately 2cms above the supra orbital rims. At this point the periosteum is
incised and the dissection is continued in the subperiosteal plane. The supraorbital neurovascular bundles are protected.
Laterally the dissection continues in the subgaleal plane up to 1-2 cms above the zygomatic arch. The deep temporal fascia
is incised at this point and the dissection continues deep to the temporal pad of fat over the temporalis muscle and the investing
fascia. The deep temporal artery perforators should be protected if not this could lead to a hallowing in the temoporal area due
to wasting of temporalis muscle.
The anterior table of frontal sinus is exposed. A window is created over the anterior table of frontal sinus using a fissure burr.
The interior of frontal sinus was visualized and the leak was identified over the posterior table of left frontal sinus which was
sealed using tissue glue and abdominal fat.
The interior of frontal sinus was visualized and the leak was identified over the posterior table of left frontal sinus which was
sealed using tissue glue and abdominal fat.

No comments:
Post a Comment